

In Guinea, Sierra Leone and Liberia, three neighbouring West African countries, Ebola seems to be out of control. This is a graph of the numbers of new cases with projections for the next four weeks in lighter blue:
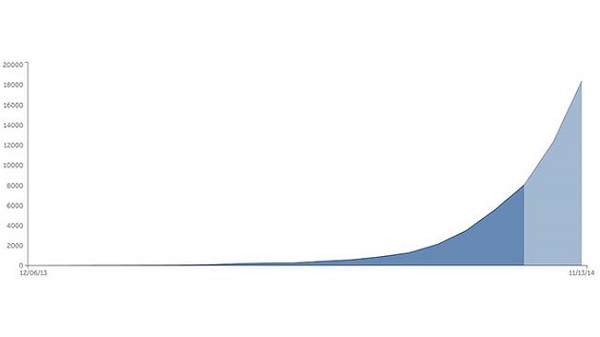
So far there have been about 8,400 cases and some 4,000 deaths. There are claims that cases in Liberia are doubling every 15-20 days while those in Sierra Leone are doubling every 30-40 days. By the end of the year there could be as many as 18,000 new cases weekly.
I’m impressed though that there has been no spread to other African countries other than Nigeria, where it appears to have been contained. One case surfaced in Lagos in July with 19 subsequent infections. However, the chain of contagion seems to have been broken.
On the other hand subsequent infections in the US, where a second health care worker has tested positive, and Spain are cause for concern.
You can read very different views of the potential impact of the disease worldwide. This Nature article is quite definite that the Ebola does not represent a global threat. The virus is too hard to catch and advanced country health systems are too sophisticted. By contrast this New York Times piece worries about the virus gaining a foothold in a mega-city somewhere else in the developing world. I’d worry about India and the capacity of its health system to cope.
The current outbreak is the first time the disease has gained a foothold in urban areas.
A second worry is that the virus may become airborne. C Raina MacIntyre, who is Professor of Infectious Diseases Epidemiology and Head of the School of Public Health and Community Medicine at UNSW, points out that experienced health care workers who have contacted the disease have not been able to identify how they caught it. The assumption is simply that there has been a breach in protocol. We keep being assured that the disease is hard to catch. While the long incubation phase, up to three weeks, does not help memory, the fact that it keeps happening in ways that can’t be precisely pinpointed is troubling.
Still, the circumstances that saw the disease take hold in West Africa are unlikely to be repeated. This Vanity Fair article explains how the spread of Ebola was assisted by unique circumstances.
Firstly Ebola was not identified for three and a half months. The disease was virtually unknown in West Africa; earlier outbreaks had been in central and east Africa. At first cholera, then Lassa fever were suspected. By the time Ebola was identified the disease had already spread to a number of towns, including a bustling trade hub.
The reaction of first world agencies was swift. After identification in late March, Guinea was invaded by strange robotic white people who came in space suits and took ill people away.
The foreigners had come so fast that they had actually out-run their own messaging: there were trucks full of foreigners in yellow space suits motoring into villages to take people into isolation before people understood why isolation was necessary.
To a villager, the isolation centers were fearsome places. They offered a one-way maze through white tarpaulins and waist-high orange fencing. Relatives or friends went in and then you lost them. You couldn’t see what was happening inside the tents—you just saw the figures in goggles and full-body protective gear. The health workers move carefully in order to avoid tears and punctures; from a distance, the effect is robotic. The health workers don’t look like any people you’ve ever seen. They perform stiffly and slowly, and then they disappear into the tent where your mother or brother may be, and everything that happens inside is left to your imagination. Villagers began to whisper to one another—They’re harvesting our organs; they’re taking our limbs.
The people in Guinea were as frightened by the response to Ebola as they were by Ebola itself. By May the cases dried up and the aid agencies started to relax. In fact the sick were hiding, as soon became apparent.
Rather than under control the reverse was true, the epidemic was completely out of control. While new strategies are gaining the trust of the people, the disease has outrun attempts to contain it.
There must be a huge effort to contain the disease within the three countries where then disease is endemic while a vaccine, currently under development, is fast tracked. As to Guinea, Liberia and Sierra Leone, we can’t just write off a combined population of over 20 million people. Health workers are in the front line and these countries human health worker resources are being depleted by the disease. Liberia has only 250 doctors left for 4 million people, that’s one for every 16,0000 people.
Yet Australia has seen no great obligation to help. Officially I understand we have supplied about $18 million in aid, a pathetic amount, while our fearless prime minister has said that it is too dangerous for us to put boots on the ground. Yet there is work to be done out of direct contact with patients, in building temporary field hospitals, for example. Our PM could show just a bit of compassion and genuine humanitarian concern.
From what I have seen (absolute non expert) this virus is very small and thin, and coated throughout its length with molecules that allow it to attach itself with ease. This means that it is very “sticky” and the reason why I would not expect it to become airbourne at all easily. But being very small this allows it to raid building materials within cells to replicate itself prolifically. I would expect that it would take only one intact virus on a new victim to become infected as long as the virus can penetrate a living cell and the cell remains attached to the victim’s body.
In the early days of ebola outbreaks the method of handling was to seal the victims into their properties and let nature take its course. Now that the aim is to attempt to save victims the risk of spread is hugely magnified as there are now thousands of exposure opportunities.
The potential of a global epidemic is serious. The real test of this is now being played out in the US. We are also seeing just how good that ultra expensive US medical system really is.
Part of the problem in Africa has been people being isolated without a mechanism to get food etc. to them. (I am talking about people who may have been in contact being isolated.) There have also been reports of people breaking into the Ebola treatment areas to get medicines etc. because the whole medical system was unable to cope with its normal load at the same time.
In theory countries like Aus have the capacity to deal with this sort of crisis. However, when you think about our waiting lists, hospitals shutting down beds etc. you wonder how much surplus capacity really is available. It is also worth remembering how some Labor governments were criticized for taking too much effort over the flu epidemic. ditto the TB related consequence of recent cutting back on our medical efforts at our Torres Strait border.
It is about time that you realise that
“Our PM could show just a bit of compassion and genuine humanitarian concern”
has absolutely non of this. Sociopaths are deficient in empathy and do not have the emotional triggers to react to the distress of others. There are more likely to revel in the suffering as this feeds into their sense of gain and winning.
It seems to me that health systems in developed countries are going to be severely tested. They have been under pressure just about everywhere. I heard that in Spain, for example, they have had horrendous cuts as past of an austerity drive, and that training in proper procedures had been non-existent.
Here a patient feeling ill would normally present at an emergency department, just about the worst place to be.
People who haven’t realised that they have been in contact with someone with Ebola are unlikely to report to doctors or hospitals simply because they have a fever. If everyone who had a fever did report the system would be swamped.
As far as I know we haven’t got a quick method that could be used for self testing.
It looks as though we may have developed a vaccine but it will take time to ramp up production.
JD,
Apparently the vaccine was developed a while ago but was not tested etc because the drug companies couldn’t work out how to make a profit from it, it had cost so much. After all it was only African blacks who were dying. – A horrifying sentiment, but apparently not that far off the mark.
I;m actually quite worried that the Abbott Government will be so incompetent, if there is a crisis it will get out of control, but not completely out of control. They’re already on record over this about ignoring the AMA.
We need Nicola Roxon back as a matter of urgency. Dutton……….
Lol, yeh, she’d get a few more tonnes of useless Tamiflu.
And plain package it to raise it’s use in younger Australians.
Perhaps an Ebola-pops tax.
She could make it illegal for ebola to insult or offend.
Blame Kevin07 for it.
Haha, good one Dutton…..
Apparently Abbott’s reluctance to send personnel officially is based on the remoteness of West Africa. The trip back to Australia is 30 hours. Once infection is diagnosed the disease progresses rapidly and a worker with the disease would almost certainly die on the trip. Moreover the RAAF does not have the isolation facilities required to take anyone with Ebola anywhere.
West Africans contracting the disease have about a 70% chance of dying. While there are no specific treatments, modern hospital care can reduce the mortality to somewhere around 50%.
Labor and the AMA are saying the government is being slack in it’s effort to put boots on the ground. They are being portrayed in the press as reckless. What they are actually saying is that the Government should be making arrangements with the Europeans and/or the Americans for evacuation and treatment, and they are leaving it up to the public servants rather than take it up at the political level.
There are legal problems because most countries have immigration laws denying access to foreigners with infectious diseases.
The Brits, I understand, are building a special facility in Africa for the treatment of foreign care workers. We need to negotiate access to that.
The real question is what is needed right now and what is the best way for Aus to help. It may not be boots on the ground.
Jumpy: When we are facing something that could be a real medical crisis I like a minister who over-reacts and gets the medicines and other resources we MIGHT need..
Brian nails it.
But I have been saying for many years we need an international medical defence force.
Nations, rather than use decommissioned naval vessels target practice and artificial reefs, convert some of these ships for use in humanitarian purposes.
All the first world countries could do it.
Deck em out like mobile hospitals with some support vessels equipped to suite the catastrophe.
Crewed and funded out of aid budgets and NGOs.
What about land locked countries in need you ask ?
We there are hectares of decommissioned aircraft in the Arizona desert slowly rusting away because they’re not ” economically viable anymore ”
This could all be put together and coordinated out of the UN.
Easy peasy.
But they’re to busy fighting for transgender islamic poley bears or some such.
Id bring it up at the G20 but my invite seems to have been gobbled up by Australia Post.
Norman Swan interviewed Professor Edward Holmes of Sydney University about the Ebola phenomenon. Prof Holmes thinks it’s unlikely that the virus will become airborne, but stresses that we don’t know how infectious this particular strain is. Like influenza, as an RNA organism it changes to some degree every time it reproduces.
He didn’t comment on this specifically, but I think the biggest question is whether or not the virus needs to penetrate through an orifice or a break in the skin. I’ve read at least twice now that it does. So for example if you touched your eye with an infected glove you could catch the thing, but not by touching your cheek unless you have a break in the skin there.
This seems to me an open question.